September 2023 Case
Contributors: Julia M. Rivera-Sustache, Rachna Jetly MD, MPH
CLINICAL HISTORY
A middle-aged individual presented to the otolaryngology clinic for evaluation of a large, painless neck mass that had been present for more than five years and remained stable in size. The patient was well otherwise. On physical exam, a soft to firm mobile mass, approximately 5.00 cm, was palpated in the right neck. On the head and neck computed tomography imaging, there were multiple enlarged right anterior cervical lymph nodes, the largest being approximately 6.0 cm in greatest dimension. An initial needle core biopsy had atypical scattered large cells of a B-cell immunophenotype in a background of small T-cells and histiocytes; a definite architectural assessment was precluded by the limited nature of the specimen. A subsequent excisional biopsy revealed an enlarged, firm, 6.2 x 4.5 x 1.6 cm lymph node with a focal vaguely nodular parenchyma on cut section, and no necrosis. Both biopsies had no evidence of B or T lymphoproliferative disorders by flow cytometry immunophenotyping performed on fresh tissue. Representative sections stained with hematoxylin and eosin (H&E) and some immunohistochemical stains are demonstrated in the figures below. Architectural patterns are variable, nodular in some areas (Figure 1) and diffuse in others (figure 2).
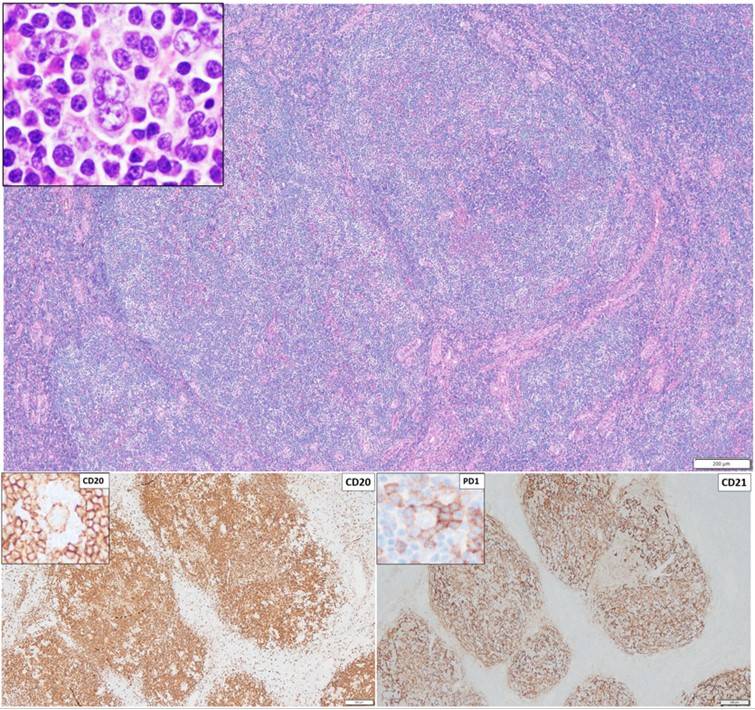
Figure 1
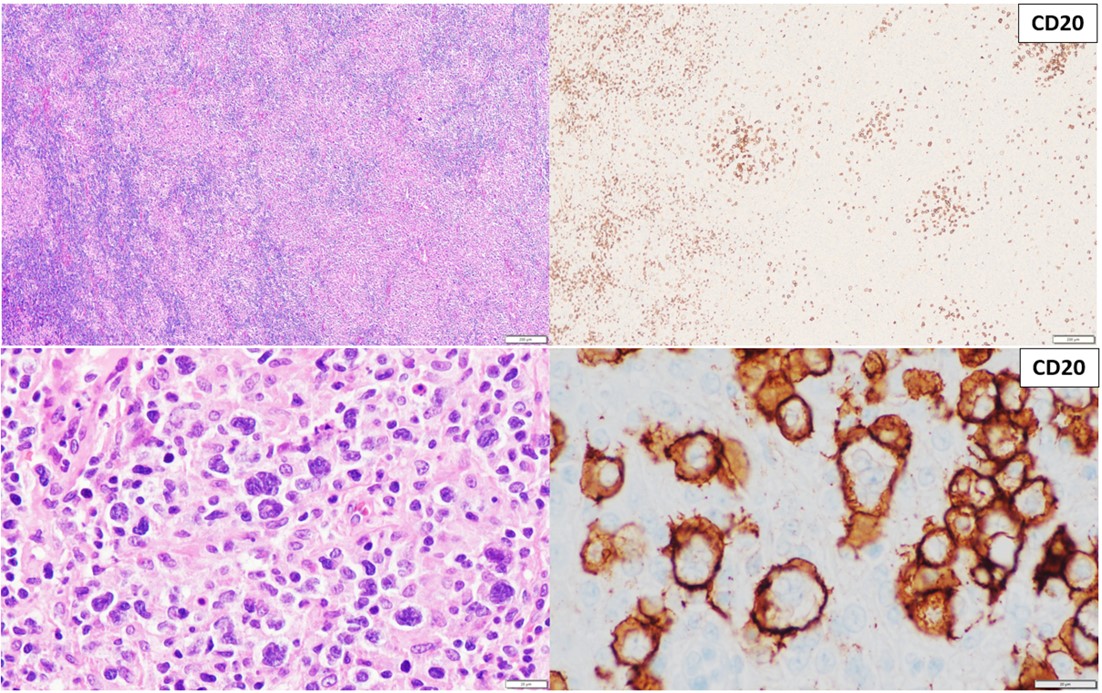
Figure 2
Based on the WHO classification of Hematolymphoid Tumors (5th edition, 2022), which
of the following is the most likely diagnosis?
A. Lymphocyte-rich Classic Hodgkin lymphoma
B. Nodular Lymphocytic Predominant Hodgkin lymphoma
C. T-cell/histiocyte-rich large B-cell lymphoma
D. Nodal T-follicular helper (TFH) cell lymphoma, angioimmunoblastic-type